



HEARING AIDS
give meaning to sounds
Hearing aids
Give meaning to sounds
The correction of an auditory deficiency reveals a multitude of aspects and parameters; from acoustic, physiological, to personal and or professional.
The Natacha Chetritt Bonneyrat’s ambition and commitment is to respond with the same professional code of ethics to all of our clients’ requests thereby making each application of an auditory aid unique.
It is within this context of respect and professionalism that we dedicate ourselves on a daily basis defending the ethical values to which we adhere, allowing nothing to re-orientate them.
Natacha Chetritt-Bonneyrat provides audiological care* only to patients who wish to benefit from highly qualified care.
You entrust one of your most precious senses to us, be assured that together we will succeed in restoring it.
Natacha Chetritt-Bonneyrat, audiologist in Cannes, offers you hearing aids combining the most advanced technologies in the world and a resolutely innovative design.
*It is imperative that any intervention for an auditory appliance must be preceded by a consultation with an ENT specialist who will determine the type and degree of your auditory loss and who will be able to assure that there is nothing to prevent you being prescribed to wear an auditory aid.

Natacha Chetritt-Bonneyrat was elected Best Audioprosthetist of France of the year 2019
by a jury of professionals Audiologist Of The Year Competition
Hear is essential, protecting your hearing is pimordial
With an exponential exposure to sound in our current society, it is advisable to adopt a responsible and reasonable “sound hygiene” in order to avoid consequences, sometimes irreversible, related to noise.
It is important to remember that exposure time can be just as detrimental as intensity.
Whatever the sound situations that characterize an attenuation of ambient noise, there is an appropriate protection solution for each situation to reconcile performance and comfort.
In order to best preserve your hearing capital, Natacha Chetritt-Bonneyrat offers you a range of 100% tailor-made hearing protection specially designed for your professional or leisure activities.
Whether it is the practice of a mechanical sport, a professional activity in a noisy environment, the pleasure of a concert, the practice of hunting or simply to neutralize the undesirable effects of pressure variations during take-off and landing in plane, but also to protect your eardrums when swimming or allow you to find a peaceful sleep…
Anatomy of the auditory system
Outer Ear
The outer ear receives sound waves (air vibrations) via the pinna and the waves travel through the ear canal to the tympanic membrane.
Middle Ear
The middle ear is made up of the tympanic membrane and the malleus, incus and the limbs of stapes forming a tiny chain of ossicles (small bones). First of all, the sounds coming from the outer ear cause the tympanic menbrane to gently vibrate. Then, the ossicles concentrate and amplify the sound’s energy by adapting its impedance, which is then transmitted through the oval window, where the inner ear begins.
Inner Ear
The inner ear contains a fluid, which carries the sound waves controlled by the movement of the oval window, which in turn stimulates the inner hair cells, inside the cochlea, generating electric impulses. This influx is then transmitted via 30,000 nerve endings which make up the auditory nerve, which in turn transport the information to the central auditory part of the brain.
The brain
Without which, nothing would be audible. The hearing brain then undertakes the specific job of decoding and interpreting the neuro-electrical impulses. It is here the auditory input metamorphoses into something comprehensible for Man. This is why it is paramount to preserve the quality of the transmission of the information signals either by respecting a safe decibel level when there is no existing lesion, or by using a hearing aid when there is an evident auditory deficiency.
Types of hearing loss
Hearing transmission loss
Auditory transmission loss is characterized by damage to the outer or middle ear. Sounds do not reach the inner ear correctly. In cases of temporary disfunction, this type of auditory loss is usually treated medically or with surgery.
The main causes are
Traumatism to the outer ear build-up in the ear canal of wax or other undesirable blockages ear infections otospongiosis perforation of the eardrum congenital malformations or after-effects of a difficult birth.
Perceptive or neuro-sensory hearing loss
(including damage to the cochlear and the integrality of the auditory system including the cortex) Neuro-sensory, auditory/hearing loss represents the majority of auditory problems and generally originates from the body’s ageing process however sound traumatisms, taking of medicines toxic to the ear, ear infections or congenital factors can also be the cause. We classify viral infections, prematurity, traumatisms after a difficult birth, congenital malformations or hereditary factors as being amongst the pre-natal causes. In this case, the auditory/hearing capacity is impacted because the ciliary cells in the cochlear are damaged and don’t transmit the neuro-electrical impulsions correctly to the brain (via the auditory nerve) which is responsible for carrying out the metamorphosis of the original sound signal into perceptible and understandable sounds to Man.
Retro-cochlear hearing loss
Is characterized by an attack on the nervous pathways.
Central hearing loss is differenciated by damage to the auditory nerve centres
Furthermore, when both transmission and perceptive types of loss are co-existant, it is referred to as a mixed hearing loss.
AUDIOMETRIC CLASSIFICATION OF AUDITORY DEFICIENCIES according to the work to work of the BIAP – International Office Of Audiophonology Scientific Company created by Belgian Royal order on march 24th 1967.
Normal or sub-normal audition
Tonal loss is no greater than 20 dB. Otherwise known as a slight tonal attack but with no major consequences.
Slight auditory deficiency
Average tonal loss situated between 21 and 40 dB. Words perceptible at normal speech level but which are difficult to hear as a whisper or at a distance. The majority of familiar noises are perceptible.
Average auditory deficiency
First degree: Average tonal loss situated between 41 and 55 dB. Second degree: Average tonal loss situated between 56 and 70 dB. The spoken word is perceptible if the voice is raised. The patient understands better by watching someone speak. Some familiar noises are still perceptible.
Severe auditory deficiency
First degree: Average tonal loss is situated between 71 and 80 dB. Second degree: Average tonal loss is situated between 81 and 90 dB. Words are perceptible when spoken loudly close to the ear. Loud noises are heard.
Profound auditory deficiency
First degree: Average tonal loss is situated between 91 and 100 dB. Second degree: Average tonal loss is situated between 101 and 110 dB. Third degree: Average tonal loss is situated between 111 and 119 dB. No spoken word is perceptible and only extremely loud noises are heard.
Total auditory deficiency - Cophose
Average loss is 120 dB. No sound is heard
Scale of sound heard
SOUND LEVELS BY NOISE ORIGIN quantified in decibels (dB)
- Proximité d’une fusée au décollage
- Avion au décollage
- Niveau perçu par le tireur lors de la détonation d’une arme à feu
- Seuil d’audition douloureuse
- 105 dB Limite autorisée en discothèque pour les sons en continu
- 85 dB le port de protections auditives devient obligatoire au travail
- 60 à 65 dB conversation à voix normale
- 20 à 30 dB Studio d’enregistrement
- 5 dB Niveau perçu lors de la chute d’une épingle sur le carrelage
Niveau
sonoreTemps maximum
d’exposition100 dB
15 minutes
91 dB
2 heures
88 dB
4 heures
85 dB
8 heures
Source HCSP
Understanding an auditory assessment
Auditory limitation definitions
To be audible, a sound frequency must be situated between 16 Hz and 20 000 Hz (for an infant) and more commonly up to 16 000 Hz for an adult patient. Below 16 Hz are infra-sounds which are imperceptible to the human ear but which can nevertheless induce physiological effects on the body. Above 16 000 Hz we enter into the domaine of ultra-sounds, which are too high to stimulate an auditory sensation.
Introductory tonal audiometry
Tonal audiometry is a subjective test, which evaluates auditory intensity. It uses pure sounds in order to determine the auditory threshold (the lowest level at which a sound is perceptible for each respective frequency tested) and is conducted in two ways: By aerial conduction with the help of a headset placed over the ears and by bone conduction through the intermediary of a vibrationary device positioned over the mastoid bone.
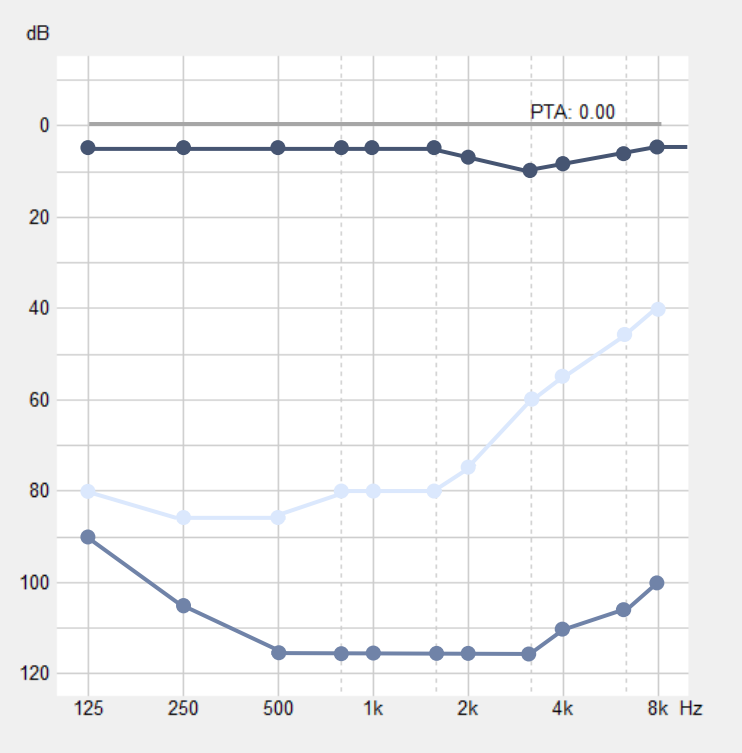
Represented in the graphic above, the corresponding values are :
Tonal audiometry reference point
Pure tone audiometry of the patient tested
Subjective discomfort threshold reference point
Subjective discomfort threshold of tested patient
Tonal audiometry supra-limitation – subjective discomfort threshold
Tonal audiometry supra-limitation in itself permits the study of the ear’s dynamics as well as the frequential and temporal selectivity thanks to the usage of pure sounds at a higher level then the auditory threshold.
This so-called discomfort is defined as the acoustic level when auditory sensation becomes intolerable.
This measure suggests to us (in the case of hearing aids) the parameters which must be considered in the settings in order to preserve the integrity of the patient’s dynamics.
Vocal audiometry
Vocal audiometry is an indispensable test, which completes tonal audiometry.
Indeed, in the areas where tonal audiometry only gives absolute thresholds of sound perception, vocal audiometry informs us about language comprehension (intelligibility) as well as discrimination (ability to discern phonemes similar).
Vocal audiometry is conducted by repeating to the patient lists of words; generally dissyllabic (Fournier), monosyllabic (Lafont) or Broomsa, designed specifically for children.
The results found dominate the indication and the choice of hearing aid and can help in the diagnosis of some retro-cochlear pathologies like, for example, the schwannome window.

Represented in the graphic above are the corresponding values :
- – Vocal audiometry reference point
- – Vocal audiometry of a patient presenting an auditory deficiency